Pediatric Apprenticeship 2024

Zoom 10
FIND YOUR AUTHENTICITY
Points to remember when things get difficult at work: We can’t control everything. Remember that our “egos” (the conscious recognition of ourselves) can be damaging to us. Don’t trash talk yourself. You are doing your best. Treating babies isn’t about remembering techniques and doing things by rote. It is about connecting to that small being, letting go, being intuitive, and following your instincts. Then apply the tools you have learned over the last several months to achieve what you need.
Technique and Palpation in Baby Treatment
Jonathan discussed the concepts of technique and palpation in the context of treating babies. He explained that technique involves doing something with the intention of achieving a specific outcome, while palpation is more about listening and observing. Jonathan emphasized that these concepts exist on a spectrum and can be blended. He also shared a case study of a 4-year-old child who was having difficulty calming her nervous system during treatment sessions. Jonathan suggested starting treatment further back, such as at the sacrum, to establish a connection and improve palpation. He also noted that asking a child to lie still can sometimes exacerbate their nervous system tension.
Osteopathic Practice: Inner Content and Transmutation
Jonathan discusses the importance of inner content as the third aspect of a triangle framework for osteopathic practice, alongside technique and palpation. He emphasizes that inner content involves connecting with one's inner life force and the divine, which can enable transmutation in patients. Jonathan stresses that practitioners should not feel limited by their perceived lack of inner content, as it is a journey of continuous improvement. He illustrates this point with a story about a student who demonstrated exceptional ability but struggled to maintain balance. Jonathan concludes by emphasizing the importance of being grounded and understanding one's practice, while also being open to relying on inner content when possible.
Spiritual Individuals in Church and Medical Cases
In the meeting, Jonathan discussed the importance of spiritual individuals in a church who perform service and cleaning, rather than being the hero. Joanne and Jessica shared their experiences and challenges, with Jessica describing her case of a child with a cleft palate and health issues. The child was treated for sinus issues and tethered tissue, but faced complications during a tissue tie release procedure. Jessica sought advice on how to handle the situation, particularly the parents' insistence on post-stretch exercises despite the child's trauma.
Tongue Tie Procedure Risks Discussed
Jonathan discussed the challenges faced by parents with a child who underwent a tongue tie procedure. He suggested that the parents were over-exerting themselves, likening it to running an ultra-marathon instead of a marathon. Jonathan advised a frank discussion with the parents, suggesting that the tongue tie procedure was not a good idea and that they should stop doing the stretches. Joanne shared recent news about a baby's death in Montreal due to a tongue tie procedure, emphasizing the importance of proper qualifications and caution when referring to practitioners.
Balancing Technique, Palpation, and Inner Content
Jonathan discusses the importance of continuous improvement in osteopathic practice. He introduces a triangle concept with technique, palpation, and inner content as the three aspects practitioners should balance. He encourages practitioners to assess where they currently work within this triangle and where they aspire to be, noting that there may be a discrepancy between the two. Jonathan emphasizes the need for deliberate practice, courage in self-assessment, and kindness to oneself during the learning process. He outlines five key points for improvement: courage to evaluate one's work, assessing results, being kind to oneself, course-correcting based on self-appraisal, and asking for help when needed.
Improving as an Osteopath
Jonathan discusses strategies for improving as an osteopath and growing one's practice, particularly when treating babies. He emphasizes the importance of balancing palpation skills, technique, and inner content. Jonathan advises practitioners to seek guidance from a higher power or their intuition to become better practitioners. He explains the concept of capacity, noting that practitioners should be aware of their limits and how their personal lives may affect their professional capacity. Jonathan also provides practical tips for growing a practice, such as having a suitable treatment space, rebooking patients, charging appropriately, and networking. He stresses that while creating a pleasant environment is important, patients ultimately come for the quality of treatment rather than the decor.
Baby's Facial Tension Improvement
Jessica presents a case study of a baby she has been treating since two weeks old, now four months old. She shares photos showing the baby's progress over multiple treatments. Initially, the baby had significant tension in the head, a small left orbit, and a pointed chin. After two treatments, there were noticeable improvements in the baby's facial features, including more space around the left eye and a less pointed chin. Jessica notes ongoing issues with eye congestion and a possible left eye turn. She also mentions the presence of a lip blister, potentially indicating a lip tie. Despite these challenges, Jessica emphasizes the significant positive changes achieved through treatment, even without addressing potential ties.
Zoom 9
FIND YOUR AUTHENTICITY
Points to remember when things get difficult at work: We can’t control everything. Remember that our “egos” (the conscious recognition of ourselves) can be damaging to us. Don’t trash talk yourself. You are doing your best. Treating babies isn’t about remembering techniques and doing things by rote. It is about connecting to that small being, letting go, being intuitive, and following your instincts. Then apply the tools you have learned over the last several months to achieve what you need.
Jessica had a question about the interconnectedness between mother and baby. Nervous system and energy.
—> Does Jon recommend treatment to the family “system”?
His answer: He has usually treated the mother through the pregnancy, thus a connection is made that way. Of course it’s always nice to be able to treat the pair, oftentimes we get moms to start treatment with us as new patients once their babies have been tended to. In other cases, we need to remember that parents are sometimes reluctant to have treatment. If this is the case (or you get that feeling) you can still create this “connection”. Jonathansuggested, as baby is cradled in mom’s arms, you can gently ask if you can lay one hand on her (shoulder or mid back) while the other is on baby, treating. “To create a comforting environment… then my attention is on both of you, and baby can pick up on that energy”. (As an example).
Kelly had an update about the unsettled baby she saw several weeks back. In tutorial #8 she had confessed to having some difficulty, which we have all experienced at one point or another. Kelly had found an interesting way to settle baby, to get “in”. She had placed her hand under baby’s sacrum and gently jostled back and forth. The baby finally relaxed and Kelly could make
some wonderful changes!
Great work! … Be authentic!
Jon discussed several strategies for “digging on”. He used case studies to make these points relevant.
Another question from Jessica about “smelly farts”. Some do smell really badly, does this mean
something? Certain foods pass some elements through breast milk which could cause this but persistent issues may indicate poor assimilation of nutrients. Think about asking if anti-biotic use was in the mom (nursing) or baby and if there could be a role for a referral out to naturopathic for prebiotic or pro-biotic treatment.
See you on Wed March 5th at 7pm for zoom 10. DO YOUR THING!
Zoom 8
Jonathan returned back to the topic of physical (briefly) and emotional fulcrums (our main topic today).
Physical fulcrums are the contacts we tangibly use to secure our positions of ourselves to the ground through our feet, our arms by our sides, our contact to our treatment tables if needed (the “bench”, as Jon calls it), and our physical touch on the patient.
Emotional fulcrums are a little more hard to describe as they relate to our non-tangible elements. For example, our emotional and energetic spaces within ourselves, those of the patient, and the meeting of all of these in between, when we enter the part of the treatment that Jonathan calls “being in service”… when we connect.
Question from Kelly about her very first baby patient, a 1-month old she treated recently. It wasn’t easy and Kelly bravely admitted her feelings about this experience. A perfect question for our palpation theme today, which Jon refers to at several points in the video.
Back to the emotional fulcrums in relation to treating a baby that is heightened energetically and emotionally from a traumatic birth experience…
When this happens they may cry very hard, arch into extension, and not allow you to treat directly with hands-on. Treat further away, distant to the body area (usually skull but could be sacrum, hip, depending…). Move just above the baby’s skin, feel for that energy field. Come away slowly and try to palpate when it wanes or decreases. Go back and forth slowly to find the best energy fulcrum that seems to tell you it is appreciated/wanted/needed by the baby. Jonathan refers to this area as the “zone of transition”. Follow what it wants. Hold space for the baby and mother’s traumatic experience. Acknowledge it and look for restful responses in the baby (body relaxation, crying stops, a smirk, etc…)
We moved onto cranial strain patterns, those that come from strains within the bone and those at the Spheno-basilar joint between the sphenoid and basilar part of the occiput. There are several that you can look up in the Core Syllabus or other cranial osteopathy textbooks. There are characteristics to each type that we won’t re-list here but a few specific points covered by Jonathan were:
- Intra-osseous strains happen within the same bone. Eg) The greater wing of sphenoid is “twisted” at the area where it meets the body/central part. NOTE: you can have a localized strain plus you’ll see an adaptive part, causing a continuity of strain distally. You can treat locally, distally or a bit of both.
- Midlines get interrupted by vertical or lateral SBS strains, not by torsions. The midline is the physical and non-physical centre, structural and emotional/energetic.
- With superior vertical strains you will often see a ridge at the coronal suture and the frontals move anteriorly. Inferior ones have a high vertex, there’s an angled look to the head.
- Many more details can be viewed in the video.
We covered more helpful information on Kelly’s 1 month old baby, who went through a traumatic birth. He was born with his right hand up against his face (explaining a R temporal area disturbance to which Kelly had a big “Ah-ha!” Moment). The birth mother was whisked away from the baby for emergency care due to heavy bleeding (detached placenta). A special note is to remember about cases like these, babies feel the disconnect from their mother if separated immediately after delivery. Think of how abandoned, vulnerable, and shocked they must feel when this happens. Hold space for this trauma when treating.
Homework: Case Study videos.
Have your own case study questions (or other topics) ready for tutorial #9 on Wed Nov 13th.
Tutorial #10 will be held in mid March 2025 (away from March break).
Certificates of completion will be in your inbox by the end of November. You must contact Joanne before Nov 30th to let her know if you haven’t received it. Otherwise you must wait until the new year. Administration is closed in December.
Certificates of completion (40 hours) will be sent out by the beginning of December.
Zoom 7
When working on babies, we rely mostly on palpation because they can't speak to give feedback like an adult, and they are moving around a lot. A different way of palpating (because of these two factors) means being quieter in our minds/intent, and moving with the babies movements, as Jonathan will describe.
Question from Jessica. What toys are good for different ages? Please see the mini video put together by Joanne that accompanies the main tutorial 7 video.
Four things that make it harder to treat babies:
- They move more, uncontrolled
- They can’t verbally tell you what they like or don’t like
- The timetable is theirs (feeds, discomforts, loneliness)
- They are more sensitive than most adults
On the other hand, a positive is, you get instantaneous feedback from their tissues due to their sensitivities. You also will see the feedback right away in their behaviour, so make sure you modify what you're doing based on those things.
Jonathan spoke at length about different examples when treating difficult attributes in adults, and how to extrapolate these problems to treating babies. To make his point/s, he ran through 2 palpation exercises: one involving the clavicle, and another one (later on in the video) involving self palpation of the back of your cranium.
These rely on VISUALIZATION and FEEDBACK, and RECOGNIZING PATTERNS, treating the MACRO (example: the baby stretch course) and MICRO (details in video).
We learned about fulcrums:
- physical fulcrums and
- emotional fulcrums
Also in the next zoom, we will learn about treating “the shock”.
Homework: Module 9 of Core Syllabus: Treating the Cranium
Toys, please see below for a video from Joanne on toys, and below that you can see a picture of Joanne's clinic toys.

Zoom 6
Video and Audio From 14th July 2023
Next Tutorial #7 Wed Sept 11th (after summer break)
#8 Wed Oct 9th (4 weeks from last one)
#9 Wed Nov 13 (5 weeks from last one) *** Certificates of completion sent!
#10 Wed March 5th 2025
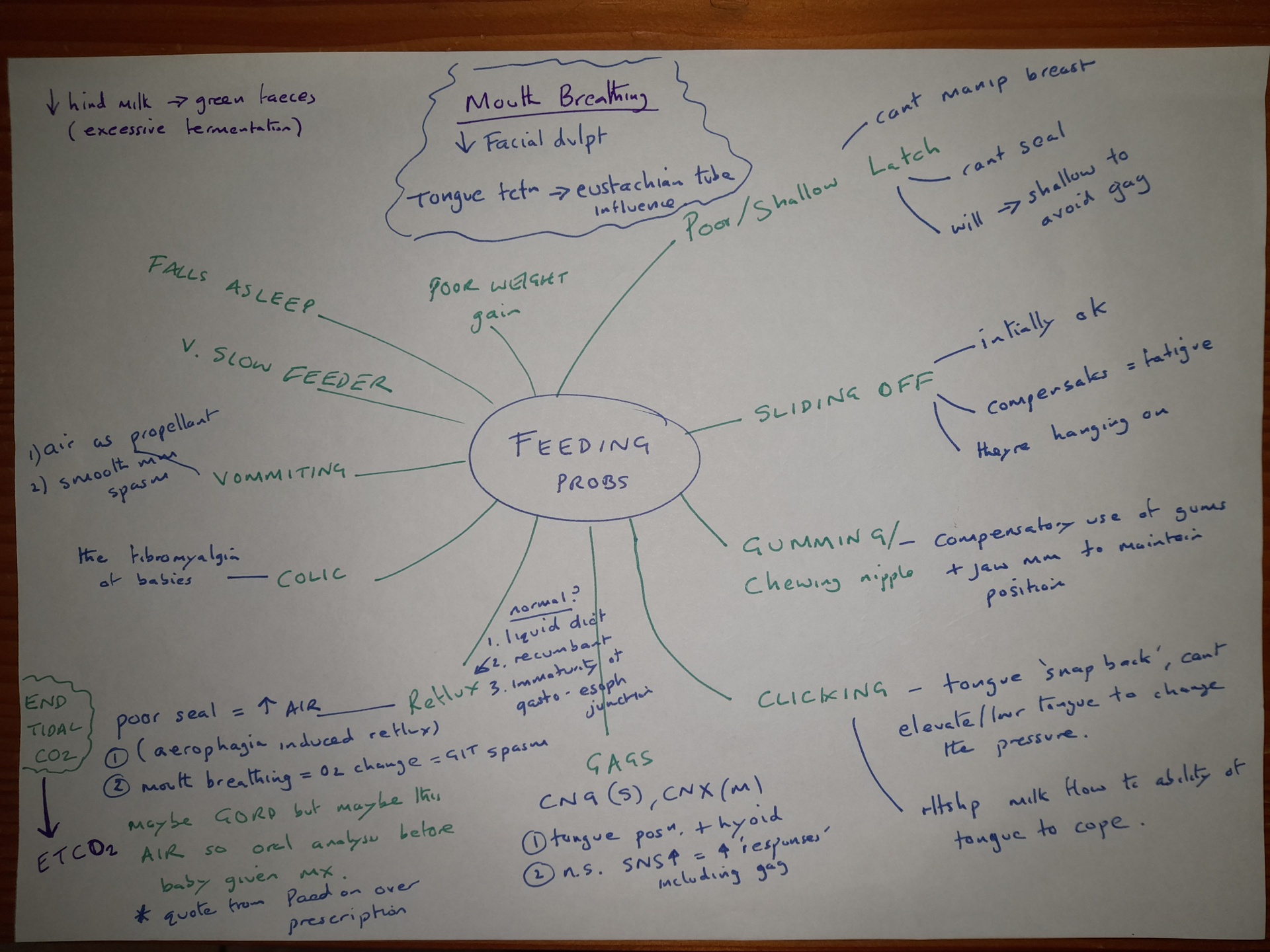
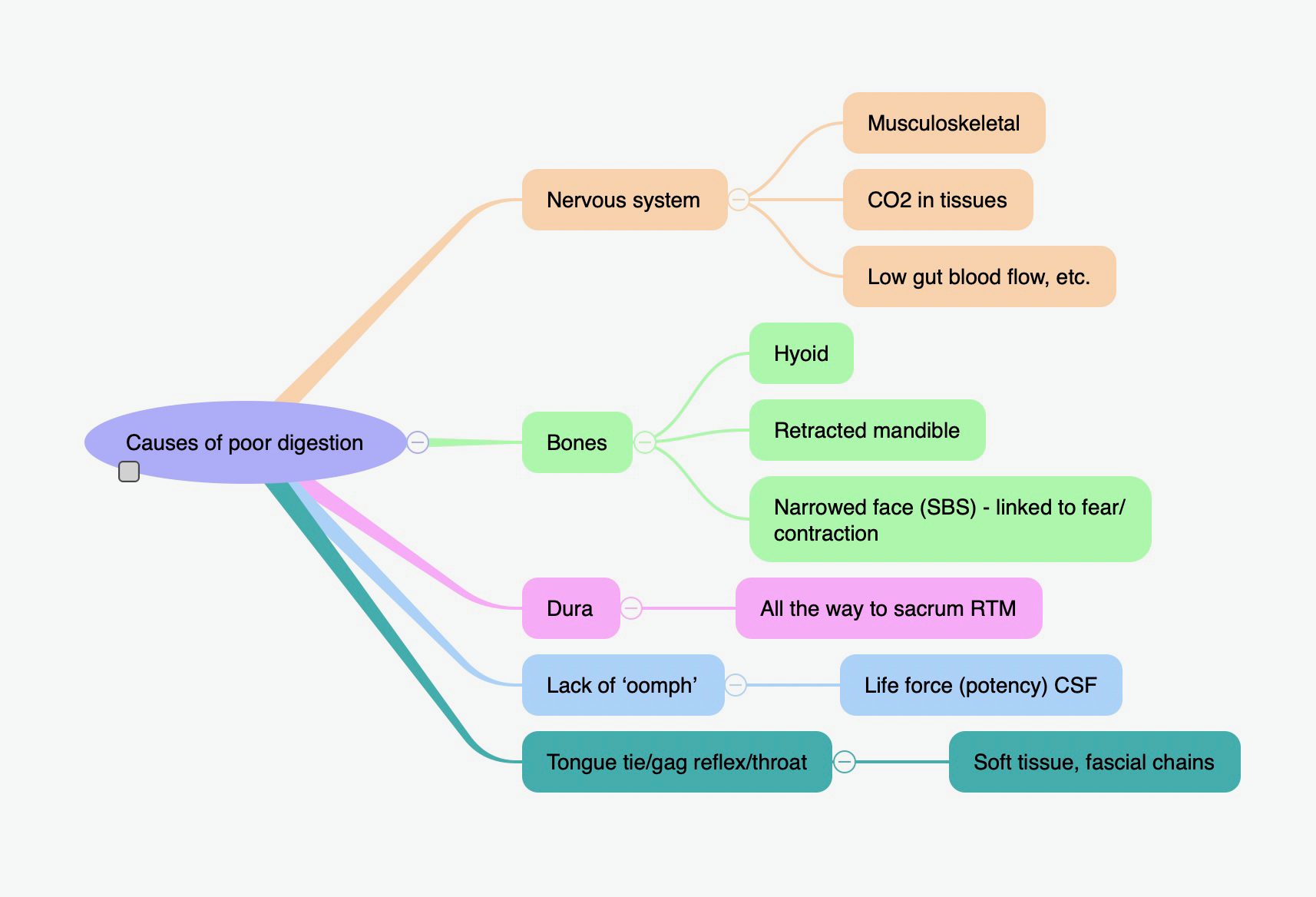
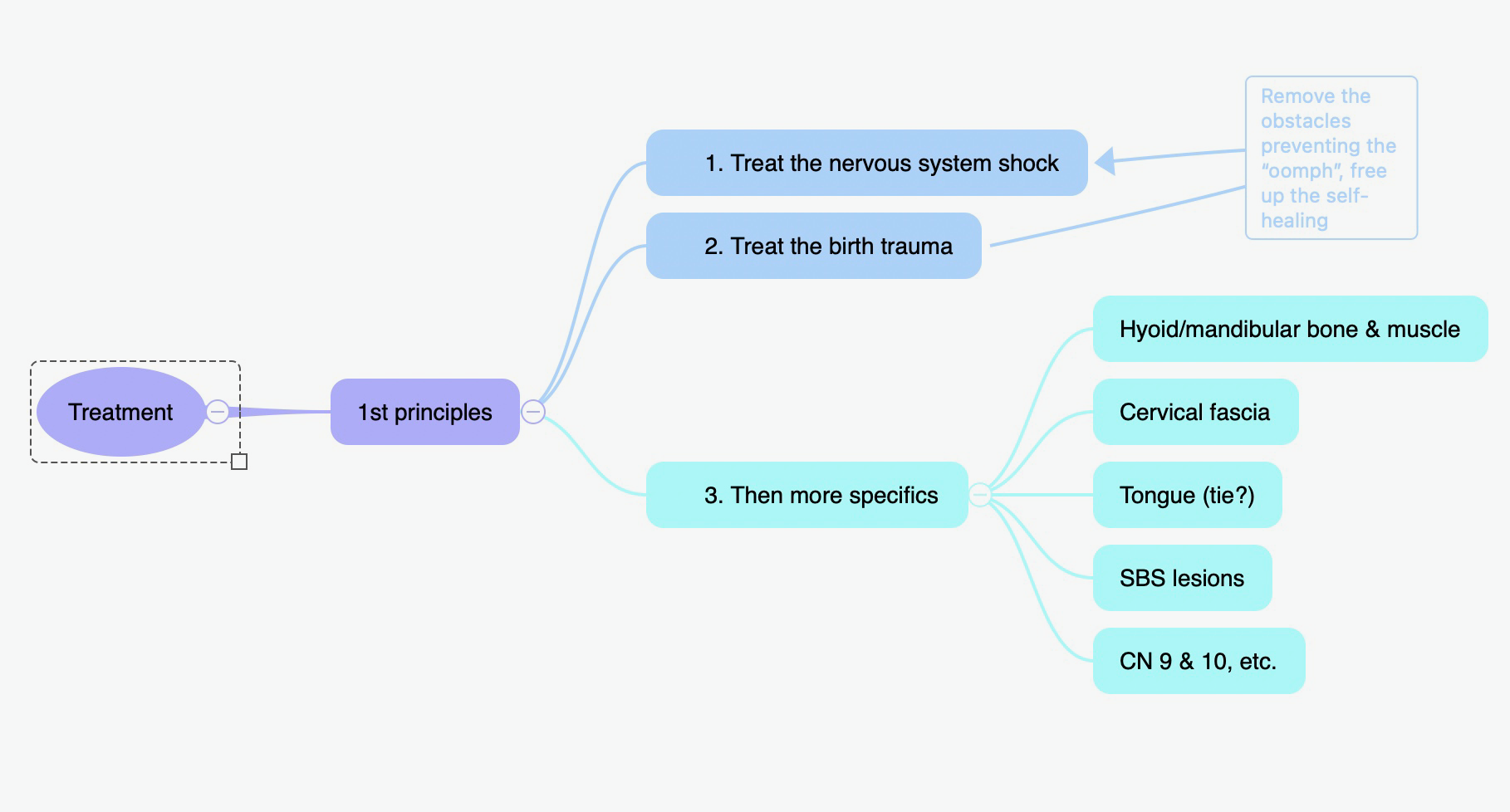
This weeks Tutorial summary notes are in the form of the above mind map.
And here's the photo of the Ethmoid see zoom for the complexity of this remarkable bone that I spoke about there.
Homework before next zoom is Module 8 Treatment Techniques.

Zoom 5
This weeks Tutorials notes are below in the form of Mind Maps, big thank you to Joanne for doing those.
Zoom 4
Tutorial #4 Notes: Examination of the Cranium
We began with a student question from Jessica regarding a retained placenta (spoken about in the Core Syllabus, history taking section). Jonathan explained always trying to look for the “why”. An unsettled baby may have an energetic or emotional attachment that was interrupted at birth (see video).
Conceptual and Practical thoughts on treating the cranium.
What do I think is happening?
Why do I think its doing that?
What can I do about it?
If by doing that, am I causing a problem elsewhere?
- Don’t start at the cranium, generally.
- Make good use of observation. This sets you up to spend less time hands-on.
- Modify your touch and meet baby where they are at, don’t push your agenda.
Irritated cranium? Baby’s energy won’t tolerate hands on their head?
—Treating “hands off” - literally just float your hands close to the cranium (how close? This is variable depending on each case). Have the child sit in parent’s lap, playing with a toy. Stand behind the parent with your arms over their shoulders and hover your hands over the baby’s head, contact the head, if possible, just take your time.
Know your anatomy! So important to understand - allow your hands to be the antennae of knowing what’s there.
“Being a cranial Osteopath”… you don’t need to be able to palpate cranial rhythm to be a “Cranial Osteopath”. There are many rhythms, and some practitioners are actually feeling their own rhythm that is matched by the baby’s or they are imparting their own rhythm to the baby.
Explain to parents, how things below, lower down in the body, can influence what is above. Especially when the head is so sensitive that the baby won't tolerate treatment directly on there.
Head shape influences: muscles, fascia, tentorium/reciprocal tension membranes, blood/fluid. Bones, like the sphenoid can be warped at ossification centres, or at the wings, that's called an intraosseous strain. Occipital bone has squamous parts and condylar parts and they're separated by cartilaginous areas. These areas need to be balanced out because they receive strains from birth.
The nervous system obviously has big influences on what we are doing. The lamina terminalis is the spot where there is convergent and divergent in the nervous system.
The heads are very resilient in babies and children. That's not to say they don't need treatment. But kids that bang their heads on purpose, kids that act out, are often very compressed in their systems…and it's like they are trying to match the compression that they FEEL. So when treating kids like this, try to match the compression with your intent, and not just physically.
Occasionally head banging can be a child wanting attention, or that they are so emotionally distressed that there is a need to do something dramatic, however this would need to be a child of an age that is aware that head banging gets a lot of attention, and even then it may still be compression rather than an emotional cause. Of course both reasons can be present at once.
Jonathan gave us a review of sphenobasilar joint strains using his magnetic skull model. Don't think too much about what it is or naming it because it can throw off your treatment. Just listen to your hands and ask the system for what it wants and needs.
No set homework before next zoom, as we want to give a chance for any of you who haven’t done up to Module 6 of Core Syllabus to catch up with that.
However, anyone who wants to do more please feel free to go through Core Syllabus Module 7 Treatment Principles and Module 8 (which is a big module) if you feel you are itching to get into the technique side of things and put those techniques into action with babies you are seeing. Remember the homework we set is just a template, so do less of it or more depending on how that suits your current home/life situation.
Zoom 3
Attendance 10/12 present today
Please remember the July tutorial has been changed to Wednesday July 3rd at 7pm (one week earlier than previously announced. It will be 3 weeks after the June tutorial).
Seated and supine examinations and dealing with unsettled babies
8 key positions
8 key transitions
Core examination is often in supine position.
Key: Observe the baby at all times for signs of agitation and to notice cues that may be helpful in your diagnoses.
"Palpation Commentary" Fill the space with your verbal explanations to baby as you keep baby engaged and keeps parents knowing what is happening.
Baby can feel abandoned if you talk to parents about unrelated things while working on baby and start to fuss, feeling resentment, wants mum (and often also your attention back.
Be the “fulcrum in the room” for yourself, for mum and for baby.
Seated examination - great to switch things up and great for thorax/rib exam, shoulder work, cranial too. The only issue is you can’t watch babies face. Ask parents for feedback if they see baby looking upset, if they spit up. Or try to feel changes in the babies body that indicate the need to change position or goal.
Breastfeeding treatment keeps baby still and quiet and you can assess latch and swallowing. It’s one of the best times to feel cranial structures too.
With fussy babies, try to crowd out the stimulus with different touch, movement. Think about what you do if you bump your elbow to inhibit the pain…. you may rub it to try to dampen the pain input with other sensation input. This sometimes works when changes in position won’t.
There was a question about head lag, when to test it (awake or asleep?) We test it when they are awake.
Please watch the "pathways" video below it is an excellent resource for understanding what is typical v atypical head lag. The whole of this Youtube “Pathways” channel is in fact really excellent as a resource.
Homework: Modules 5 and 6 from the Core Syllabus. Try not to let the homework build up! Each tutorial adds more to the homework videos so you can get the most out of your learning experience :)
Below is the video I refered to in the zoom, there are also other videos up there on the Pathways YT channel whichyou'll find useful. 3min30 in this video is head lag but it's worth watching the whole video.
Now there's a lot in these Pathways videos so dont feel you need to remember it all, or do all the positions they show in the video.
Remember once you've watched the videos, atypical development will be obvious to you when you see it in clinic.
Also remember the baby in this video is 2 months old, so babies younger won't have as good control as shown in the typical baby, there will be more lag, however not as much lag as the atypical baby. Also with that younger baby they will have some engagement of shoulder girdle, again less than typical 2 month (kind of obvious!) but more than the atypical baby shown. Final point to make is that a baby much younger than 2 months way have very similar position of head to this atypical 2 month baby when in the seated position with head dropped forward, simply because the head is heavy and they arent yet old enough to have developed enough muscle strength to lift it up (shoulder engagement wont help in this position!) It probably wont be quite as flexed as atypical baby, but it will be in a similar flexed position.
When you're in clinic if you aren't sure then its nearly always borderline eg there's something going on but its not clear cut. With those babies we record that in our notes, bring that in to what we treat and and when appropriate refer. We can dicuss these borderline cases more in later zooms and if you have a cases where you arent sure about this area please bring the case details to the zoom and we can discuss, dont be shy everyone will benefit from your case not just you!

Zoom 2
There has been ONE CHANGE to the tutorial schedule.
#2 Wed March 20th 7:30 pm (4 weeks from last one)
#3 Wed April 17th 7:30 pm (4 weeks from last one)
#4 Wed May 15th 7pm (4 weeks from last one)
#5 Wed June 12th 7pm (4 weeks from last one)
#6 Wed July 3rd 7pm (3 weeks from last one)
SKIP AUGUST (Summer break)
#7 Wed Sept 11th
#8 Wed Oct 9th (4 weeks from last one)
#9 Wed Nov 13 (5 weeks from last one) *** Certificates of completion sent!
#10 Wed March 5th 2025
ZOOM 2 Notes
Taking a history. Provide space, feeling of ease, allow mom to tell her story. Ask “how can I help”? Make eye contact, make most of your notes later, use paper and be brief unless you’re a fast typer and can maintain eye contact.
Watch the history videos in the homework, great stuff!
With Follow-Ups, Jonathan pointed out to avoid playing “tennis” if parents come in reporting baby same or worse, i.e don’t get into an adversarial experience. Stay calm, don’t defend, just acknowledge what they are experiencing, try to triangulate any issues.
A case example to illustrate important points in history taking
Jonathan treated a 2 month old boy with head bruise and minor bowel symptoms. No midwife
present for birth, a doula at a home birth. Jonathan checked to see if the head bruise had been assessed (he’d had an Ultrasound) and Jonathan also stressed to use the need to check hips in babies, especially as (1 in 100 can have an issue
“Approx 1 in 100 infants will need treatment for DDH
Hip Dysplasia: we watched two videos on Barlow and Ortolani tests.
Observation: Look at fat folds, should be equal on both proximal thighs but they won’t look equal if the hip is dysplastic..
Hip dysplasia has a family history/genetic component, first pregnancies, females,
breech babies and higher birth weight babies have higher chances.
Approximately one in every 600 girls is affected, compared to just one in 3,000 boys. The left hip is affected three times more often than the right hip.” https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/developmental-dysplasia-of-the-hip-ddh
Next, we briefly spoke about Cranial Hematoma’s. 5 types: and some references is you want more detail on them
1. Caput succadaneum - not serious, located in the skin layer, goes down quickly, can cross the sutural lines
2. Cephalohematoma - occurs in b/w the periosteum and bone layer so it can’t cross the sutural lines, these happen with hard deliveries, head jammed against bones https://www.ncbi.nlm.nih.gov/books/NBK470192/
3. Subgaleal - found below the galea aponeurosa, occurring more from harder trauma,possibly forcep deliveries https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8143819/
4. Epidural hematoma - quite traumatic, falls or blows to the head, brain damage
possible https://www.karger.com/Article/Abstract/514810
http://www.cerebralpalsysymptoms.com/brain-injury/epidural-hematoma/causes
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4315626/
5. Subdural hematoma - “shaken babies”, brain damage v likely.
Homework done before for next time if you can:
1. Core Syllabus Modules 1-4 (I said modules 1 - 2 in the zoom, that's incorrect please if you have time do modules 1 - 4)
2. Get your hands on babies to practice your new skills
Remember to turn off your negative, self-defeating thoughts, TURN THEM OFF :)
They are unhelpful. Turn your attention into your hands and listen to what the baby’s body is telling you whenever doubt enters your head. Keep switching positions when they fuss, give them a break with Mum/other parent, resume, diagnose things while baby lies in their arms, sit them up to face Mum/parent, etc…
Zoom 1
Zoom 1 Notes from Joanne
Wednesday February 21, 2024
Cohort 2024 Tutorial #1 Attendance 10/12 present today
We began the tutorial by voting for future zoom date planning. That said, the majority indicated Wednesday evenings work best. Feedback from some group members requesting all zoom dates be announced for better planning. The schedule is as follows:
#2 Wed March 20th 7:30 pm (4 weeks from last one)
#3 Wed April 17th 7:30 pm (4 weeks from last one)
#4 Wed May 15th 7pm (4 weeks from last one)
#5 Wed June 12th 7pm (4 weeks from last one)
#6 Wed July 10th 7pm (4 weeks from last one)
SKIP AUGUST (Summer break)
#7 Wed Sept 11th 7pm
#8 Wed Oct 9th 7pm 4 weeks from last one)
#9 Wed Nov 13 7pm (5 weeks from last one) *** Certificates of completion sent!
#10 Wed March 5th 2025 7pm
These are booked to maintain appropriate timing 4-5 weeks apart and to avoid the many summer national holidays we have.
Remember, the Apprenticeship Page (i.e. this page you are on will have all the zoom recordings as well as an audio only version of the zoom in case that’s more convenient for you, zoom notes, & special interest information. This page is accessible via this link https://www.kindredbe.com/2024-ax-pediatric-apprenticeship which we recommend you bookmark in your browser. Note this page is password protected. If you are already logged in to Kindred Academy you will go straight to the page, if not it will ask for your Kindred login and password.
That link will also be included in the post zoom emails after every zoom event. The zoom emails are sent approximately 3 to 4 days after each tutorial to allow for uploading of the recording and creation of the audio version etc.
NOTES FROM ZOOM 1
Jonathan reviewed how the kindred courses work and reminded everyone that there is unlimited viewing of this content, in perpetuity. We are always here for you! It is a supportive experience no matter when you need us.
How we approach treating babies:
- We get instant feedback from babie’s, less so from adults, so listen for that feedback, especially little signs, before baby gets upset. Pay attention and listen to your hands
- Wait longer, hold your hands in one place longer, give attention to the tissues in order to make a great connection
- We must watch for signs of restriction and discord in the baby’s nervous system and tissues. They can show us in subtle ways that something is caught or restricted or bothering them, and that may include us! As sometimes its our touch or intent that is bothering them, especially on a sensitive part for them.
We watched a video of o Baby in Hospital in the SCBU.
Jonathan explained some aspects of the Baby Stretch course. When we stretch a baby’s limbs, torso/body, we stretch with attention and active listening. We maintain a big picture in our minds of what's happening internally; with the nervous system, breathing, and emotional holding, etc…
Stretching for babies has 3 levels
- A) "Just Stretch - like mum or dad would do for baby if you showed them
(Although it's really never just stretch! Even when untrained mum or dad does it)
This will hugely help baby, remember if we free up the body a little it will help with breathing and baby breathes 1mil in 1st 3 weeks!
Movement is life, you know this, whether its blood flow, lymphatics, other major systems,
- B) Stretch with attention, Active Listening
its not just stretch when you do it cos you have palpation skills, you are actively listening, when you put your hands on.
You are treating even if your hands don’t move and you don’t think your treating!
- C) Stretch + Active Listening + Focus on Big Picture Internals
With our intent we can focus on various aspects whilst we're doing the stretches eg M/L, nervous system, inertia in the system, force vectors, Emotional holding, breathing etc.
We watched “Mod 2 video 4, Perfect Communication”. Jonathan showed nice baby stretch technique as a baby slept. You can use the Baby Stretch technique when you
- don't know where to start
- when your energy is poor, either emotionally or physically or mentally
- when you are just getting comfortable with babies
Jonathan reminds us to bring up our minimal level. As practitioners we want to keep getting better and better, keep making improvements in our methods of practice. We always want to see improvement in our minimal level of success, rather than expanding upon or trying to increase the frequency of our highest levels of results.
We then watched the video The three RRRS. Range, resistance, response, symmetry. Jon discussed using these tools and principles with babes.
Dealing with parents: treating and being asked questions can be difficult, deal with this by
- Accepting you will never know everything and that's OK.
- Understanding your audience and modulating your language so it suits that audience.
- Palpation commentary.
These tactics help you ‘hold the room’.
We watched a final video “Creating Slack” to get an idea of what's coming up in future tutorials.
Jon discussed different types of technique and showed us a scale, a range between structural and energetic.
Where do you currently sit on the scale? Where do you want to be?
The more broad you are along the spectrum the more tools you will have to help you treat effectively and successfully.
Question from Jessica. Is it helpful to practice on adults if we don't have babies to practice on? For the baby stretch techniques? (watch video).
Question from Sofia. Could you clarify what we will be learning about biodynamics? Long explanation (watch video).
Question from Sharon. What age range are we learning to treat? 0-18 months. Although can use skills learnt in apprenticeship for older eg toddlers but they’re a much tougher crowd!
